An echocardiogram (or echo) is an ultrasound-based test that can tell us a great deal about your heart. By bouncing and receiving ultrasound waves off your heart and adjacent structures, we can generate images of your heart. We can learn about the size and function of the right and left side of your heart and the valves. We can estimate pressures but not directly measure pressures. As we have emphasized in many different places on this website, an echocardiogram is not a substitute for a right heart catheterization. The diagnosis of PAH should never be made without a right heart catheterization and treatment should not be started until after a right heart catheterization is completed. Let’s take a more detailed look at the components of the echocardiogram report.
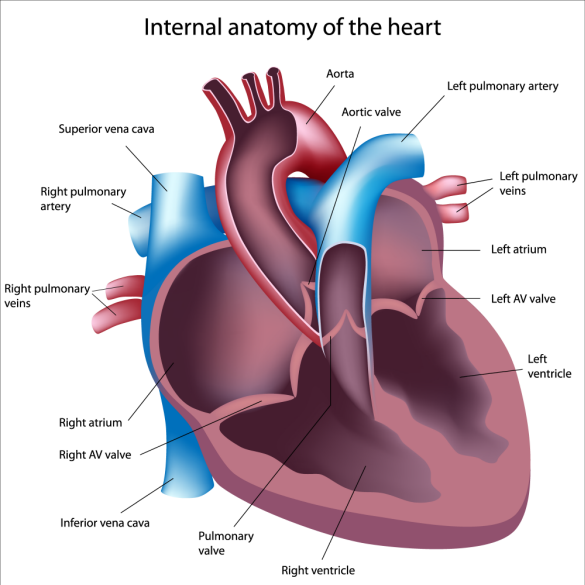
Left Ventricle
This is the chamber that pumps blood full of oxygen into the aorta and throughout the entire body. The report should describe the size of the left ventricle. The walls may be normal in size, too thick or too thin. The squeeze of the ventricle is referred to as the Ejection Fraction. A normal ejection fraction is > or equal to 55%. This is the pumping capability of the ventricle. The relaxation phase of the ventricle is described by it’s diastology. This is much harder to measure accurately. Even when measured properly, the echo may miss major problems with the way in which the left ventricle relaxes. Unfortunately, many reports omit this section.
Left Atrium
This chamber receives oxygenated blood from the lungs and conveys it to the left ventricle. The report should describe the size of the left ventricle.
Right Ventricle
This chamber pumps blood that is depleted of oxygen to the lungs where the blood will pick up oxygen. It pumps into the pulmonary arteries. The report should describe the size and function of the right ventricle. The shape of the right ventricle is more complex than the left ventricle so that a simple measure such as ejection fraction is generally not used. The walls are described as normal, too thin or too thick.
Right Atrium
This chamber receives blood depleted of oxygen from the body and conveys it to the right ventricle. The report should comment on the size of the right atrium.
Valves
There are four valves in the heart. On the right side the Tricuspid valve separates the right atrium and ventricle (top and bottom chambers on the right side). The Pulmonic valve separates the right ventricle and the pulmonary arteries. On the left side of the heart, the Mitral valve separates the top and bottom chambers and the Aortic valve separates the left ventricle from the aorta. A detailed echo report should describe the function of each valve. Any degree of leakiness or narrowing should be commented upon and quantified.
Estimation of Pulmonary Artery Pressure
By measuring the velocity of blood that moves backwards across the Tricuspid valve, the echo can estimate the pressure in the pulmonary arteries. This relies on a modification of the Bernoulli equation. The equation is as follows:
Pulmonary Artery pressure = 4 x (TRV) 2 + RAP
TRV= tricuspid regurgitant velocity
RAP= Right atrial pressure
Why is the pulmonary artery pressure that is estimated by echocardiography often inaccurate?
The key to understanding this lies in recognizing the sources of error.
1. The tricuspid regurgitant velocity is often very subjective. It depends on the quality of the echo images, the echo technician and the size of the patient and the amount of lung disease that the patient has.
2. The right atrial pressure can only be roughly inferred from characteristics of the hepatic veins and the inferior vena cava. Many labs just use 10mmHg. This practice is to be discouraged as it is rarely the best estimate of right atrial pressure
In patients with advanced lung disease, the pressure estimates are accurate about half the time.
Bubble Study
This helps identify holes in your heart that allow blood to pass from the right side to the left side. A small intravenous catheter is placed in your vein. 9cc of saline and 1 cc of air are agitated together to create tiny bubbles. These bubbles are then injected vigorously into your vein. The bubbles should travel through your superior vena cava into your right atrium, through your right ventricle and be trapped in your lungs. If any bubbles are seen on the left side of your heart, there must be a communication. The most common communications are at the level of the atria (top chambers) and are called either persistent foramen ovale or an atrial septal defect. Less commonly, the communication may be between the ventricles and is called a ventricular septal defect. Another source of right to left communication is through abnormal vessels in your lungs (arterial-venous malformations). The timing of the appearance of bubbles on the left side of your heart can help determine the type of right to left communication.
TAPSE
This stands for tricuspid annular plane systolic excursion and is a measure of how well the right ventricle contracts. Normal values are at least 18-20mm. Lower numbers suggest impaired squeeze of the right ventricle.
What can’t be measured on an echocardiogram?
1. The pressure in the left ventricle at the end of relaxation or LVEDP is unable to be measured with an echo.
2. The blood flow can’t be accurately measured with echo.
3. The pulmonary vascular resistance can’t be measured with an echo.