Your Questions Answered
Is there an oral treatment that can replace continuously infused therapy (Flolan/Remodulin)?
Flolan and Remodulin are also called Prostanoids. This family of medicine has been the backbone of PAH therapy for our sickest PAH patients more than for 15 years. In the past 2 years, the FDA approved 2 oral medicines that are in the same class (prostanoid and prostanoid-like). These two medicines, Orenitram (oral treprostinil) and Uptravi (selexipag), are more convenient to take but are not as effective as pump-based therapy. Many patients are eager to switch from their pump-based medicines to pills to avoid site pain and the inconvenience of having a catheter and pump. However, this is not advisable for most patients. Although in the short term carefully chosen patients may be able to switch, our experience over 18-24 months is that many patients will worsen and there is a risk of not being able to regain the lost ground with resuming pump-based treatment.
Other considerations include the fact that it is easy to miss doses of pills but hard to miss “doses” of pump-based treatment. Furthermore, many patients experience more side effects with pill versions of the prostanoid class medications than with continuously infused therapy. I am encouraging my patients to hang in there with pump-based treatments with the hope of an implanted pump becoming available in the next year. Of course, there are certain patients who have had hard to manage side effects from pump-based therapies such as refractory site pain and catheter infections who may be candidates for the oral options.
One of the most common questions that we receive from our readers is where to get high quality pulmonary hypertension care.
On a prior post we included a list of the Comprehensive Care Centers. These programs have been evaluated by the Pulmonary Hypertension Association and have deep expertise and well developed infrastructure to diagnose, treat and conduct clinical research.
Each month we receive a couple of questions about whether or not a patient should have a hole in their heart closed.
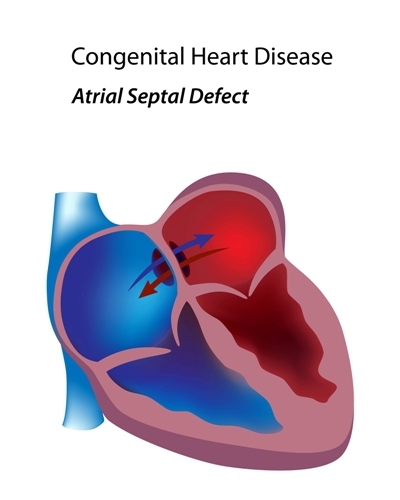
The two most common types of holes in the heart in PAH patients are called PFO (patent foramen ovale) and ASD (atrial septal defect). These are both considered atrial (top heart chamber) level communications. Cardiologists often suggest closing these holes when found. However, our practice is never to rush into closing such a hole. In general, we almost never close the smaller PFO holes. In patients with severe pulmonary hypertension we never close PFO or ASD communications. In patients with very mild pulmonary hypertension we consider closing the larger ASD communications. In patients without pulmonary hypertension, the decision to close an atrial level hole is best undertaken by a cardiologist with special training and experience in adult congenital heart disease.